
-
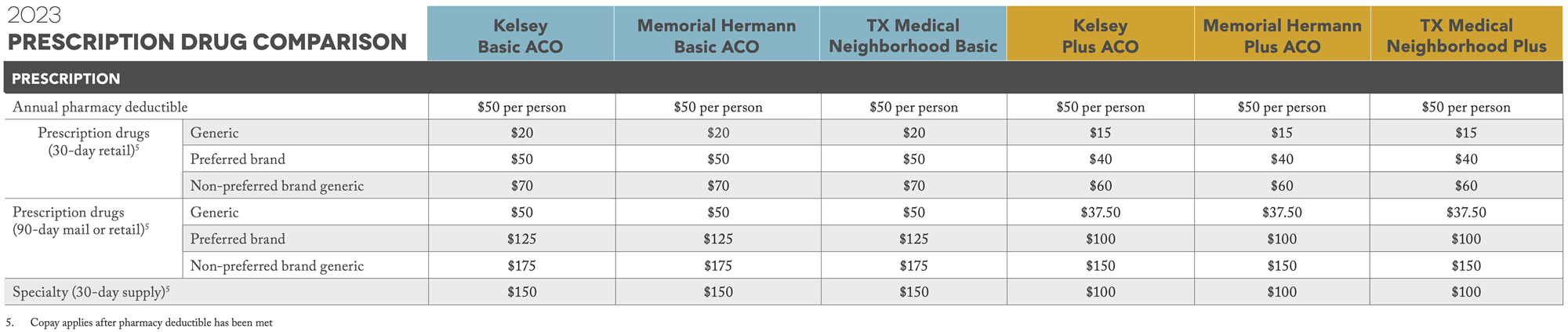
2025 coverage cost comparison
-
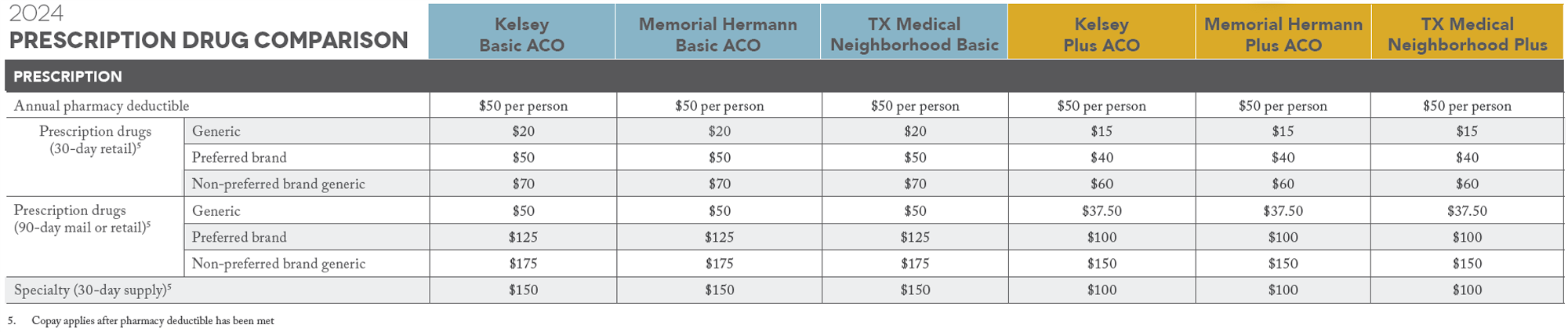
2024 coverage cost comparison
Select a School...
Select a School
- Alcott Elementary School
- Almeda Elementary
- Alternative Certification Program
- Anderson Elementary School
- Arabic Immersion Magnet School (AIMS)
- Ashford Elementary
- Askew Elementary School
- Atherton Elementary
- Attucks Middle School
- Austin High School
- Baker Montessori
- Barbara Bush Elementary
- Barbara Jordan Career Center
- Barrick (C. E.) Elementary
- Bastian Elementary School
- Baylor College of Medicine Academy at James D Ryan MS
- Baylor College of Medicine Biotech Academy at Rusk
- Bellaire High School
- Bellfort Early Childhood Center
- Benavidez Elementary
- Benbrook Elementary
- Berry Elementary
- Billy Reagan K8 Educational Center
- Frank Black Middle School
- Blackshear Elementary
- Bonham Elementary School
- Bonner Elementary
- Braeburn Elementary
- Briargrove Elementary School
- Briarmeadow Charter
- Briscoe Elementary
- Brookline Elementary
- Browning Elementary
- Bruce Elementary
- Burbank Elementary
- Burbank Middle
- Burrus Elementary
- Cage Elementary
- Career Readiness
- Carnegie Vanguard High School
- Carrillo Elementary
- Challenge Early College High School
- Clemente Martinez Elementary School
- Clifton Middle School
- Codwell Elementary
- Community Services
- Condit Elementary
- Coop Elementary
- Cornelius Elementary
- Crespo Elementary
- Crockett Elementary School
- Cullen Middle School
- Cunningham Elementary
- César E. Chavez High School
- Daily, Ray K. Elementary
- David G. Burnet Elementary
- Davila Elementary
- De Chaumes Elementary
- De Zavala Elementary
- Deady Middle School
- DeAnda Elementary School
- Distrito Escolar Independiente de Houston
- Dogan Elementary School
- Durham Elementary
- Durkee Elementary
- East Early College High School
- Eastwood Academy
- Edison Middle School
- Elementary DAEP
- Eliot Elementary School
- Elmore Elementary School
- Elrod Elementary School
- Emerson Elementary
- Energized for Excellence
- Energy Institute High School
- McGowen Elementary
- Farias ECC
- Cook Elementary
- Field Elementary School
- Fleming Middle School
- Foerster Elementary
- Fondren Elementary
- Fondren Middle School
- Fonville Middle School
- Fonwood Early Childhood Center
- Forest Brook Middle School
- Franklin Elementary
- Frost Elementary
- Furr High School
- Gabriela Mistral CEC
- Gallegos Elementary
- Garcia Elementary School
- Garden Oaks Montessori
- Garden Villas Elementary
- Golfcrest Elementary
- Gregg Elementary
- Gregory-Lincoln Education Center
- Gross Elementary
- Halpin Early Childhood Center
- Hamilton Middle School
- Harper DAEP High School
- Harris (John R.) Elementary
- Harris (Roland P.) Elementary School
- Hartman Middle School
- Hartsfield Elementary School
- Harvard Elementary School
- Health and Medical Services
- Heights High School
- Helms Elementary School
- Herod Elementary School
- Herrera Elementary School
- High School Ahead Academy Middle School
- High School for Law and Justice (HSLJ)
- Highland Heights Elementary
- Hilliard Elementary School
- Hines Caldwell Elementary School
- HISD Benefits
- HISD Human Resources
- HISD Miles Ahead Scholars
- HISD School Choice
- HISD School Website Resources
- Hobby Elementary School
- Hogg Middle School
- Holland Middle School
- Horn Elementary
- Houston Academy for International Studies
- Isaacs Elementary
- J.P. Henderson Elementary
- Long Academy
- Janowski Elementary
- Jefferson Elementary School
- John G. Osborne Elementary
- Jones Futures Academy
- Kashmere Gardens Elementary Fine Arts Magnet
- Kashmere High School
- Kate Bell Elementary
- Smith, K. Elementary
- Kelso Elementary
- Kennedy (John F.) Elementary
- Ketelsen Elementary
- Key Middle School
- Kinder High School for the Performing and Visual Arts
- Kolter Elementary
- Lamar High School
- Lanier Middle School
- Lantrip Elementary
- Las Americas
- Laurenzo Early Childhood Education Center
- James H. Law Elementary
- Lawson Middle School
- Lewis Elementary
- Liberty High School Homepage
- Lockhart Elementary School
- Longfellow Elementary School
- Looscan Elementary
- Love Elementary School
- Lovett Elementary School Fine Arts Magnet
- Lyons Elementary School
- Mabel B. Wesley Elementary School
- MacGregor Elementary School
- Mading Elementary STEM Academy
- Madison (James) High School
- Mandarin Immersion
- Marcellus Elliot Foster Elementary
- Twain (Mark) Elementary
- Mark White Elementary School
- Marshall Middle Academy of Fine Arts
- Martin Luther King, Jr. Early Childhood Center
- McNamara Elementary
- McReynolds Middle School
- Medicaid Finance & Consulting Services
- Memorial Elementary
- Meyerland Performing and Visual Arts Middle School
- DeBakey High School for Health Professions
- Mickey Leland College Preparatory Academy for Young Men
- Gulfton
- Middle College at Felix Fraga
- Milby High School
- Milne Elementary School
- Mitchell Elementary School
- Montgomery Elementary
- Moreno, Joe E. Elementary
- Henderson Elementary School
- Neff Early Learning Center
- Neff Elementary School
- North Forest High School
- North Houston Early College HS
- Northline Elementary
- Northside High School
- Oak Forest Elementary School
- Oates Elementary
- Ortiz Middle School
- Paige Elementary
- Park Place Elementary School
- Parker Elementary
- Henry Middle School
- Patterson Elementary
- Paul Revere Middle School
- Peck Elementary
- Pershing Middle School
- Petersen Elementary
- Pilgrim Academy
- Pin Oak Middle School
- Piney Point Elementary School
- Pleasantville Elementary School
- Poe Elementary
- Port Houston Elementary School
- Project Chrysalis Middle School
- Pugh Elementary
- Raul Martinez Elementary
- Red Elementary
- Redesign
- Reynolds Elementary
- River Oaks Elementary IB World School
- Roberts Elementary
- Robinson Elementary
- Rodriguez, Sylvan Elementary
- Roosevelt Elementary
- Ross (Betsy) Elementary School
- Rucker Elementary
- Sam Houston Math, Science and Technology Center
- Sanchez Elementary
- Scarborough Elementary
- Scarborough High School
- Scroggins Elementary School
- Secondary DAEP
- Seguin Elementary
- Shadowbriar Elementary
- Shadydale Elementary School
- Sharpstown High School
- Sharpstown International School
- Shearn Elementary School
- Sherman Elementary School
- Sinclair Elementary School
- South Early College High School
- Southmayd Elementary School
- Sterling Aviation High School
- Stevens Elementary
- Stevenson Middle School
- Student Supports
- Students
- Sugar Grove Academy Middle School
- Sutton Elementary
- T.H. Rogers School
- Tanglewood Middle School
- Texas Connections Academy at Houston
- Texas Education
- The Rice School La Escuela Rice
- The School at St George Place
- Thomas Middle School
- Thompson Elementary
- Thurgood Marshall Elementary School
- Tijerina Elementary
- Tinsley Elementary
- Travis Elementary School
- Valley West Elementary
- Virgil I. Grissom Elementary School
- Wainwright Elementary
- Walnut Bend Elementary
- Waltrip High School
- Washington High School
- Welch Middle School
- West Briar Middle School
- West University Elementary School
- Westbury High School
- Westside High School
- Wharton Dual Language Academy
- Wheatley High School
- Whidby Elementary
- White (Ed) Elementary
- Whittier Elementary School
- Williams Middle School
- Windsor Village Vanguard Magnet Elementary
- Wisdom High School
- Woodson PK-5 Leadership Academy
- Worthing High School
- Yates High School
- Navarro Middle School
- Young Elementary
- Young Scholars Academy for Excellence
- YWCPA
{kind=link}